
Optomap Retinal Exam
In our continued efforts to bring the most advanced technology available to our patients, Image EyeCare Optometry is proud to announce the OptoMap Retinal Exam as an integral part of your eye exam today.
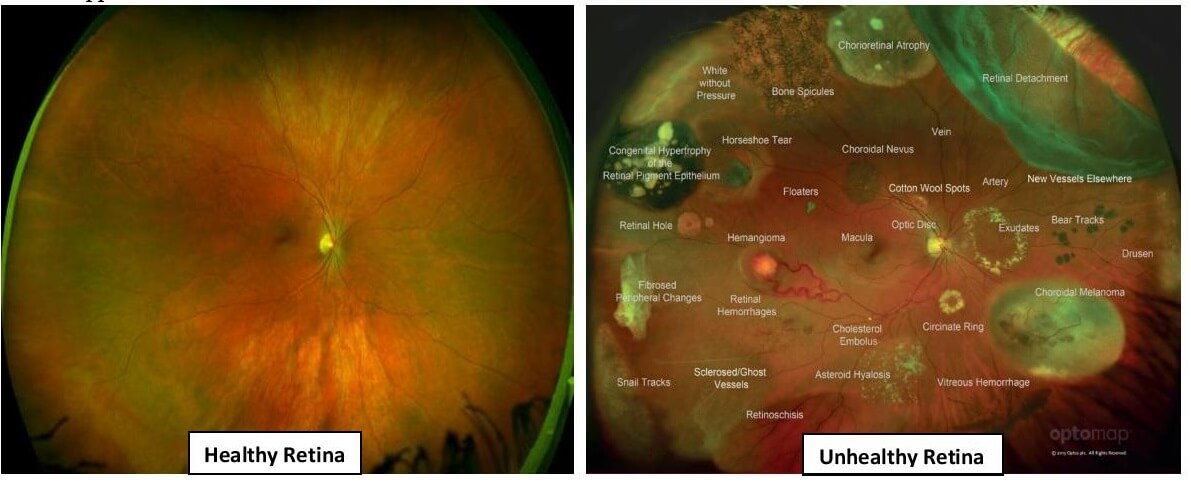
Many eye problems can develop without warning and progress with no symptoms. Early on, you might not even notice any changes in your vision. However, diseases such as Macular Degeneration, Glaucoma, Retinal Tears or Detachments, as well as other health problems such as Diabetes and High Blood Pressure can be detected with a thorough exam of the retina. The retina is the part of your eye that catches the image of what you are looking at, similar to the film in a camera.
OptoMap Retinal Exam provides:
- A digital scan to confirm a healthy eye or to detect the presence of the disease.
- An overview or map of the retina, giving your doctor a more detailed view than can be achieved by no other means.
- The opportunity for you to view and discuss the OptoMap images of your eye with your doctor at the time of your exam.
- A permanent record for your medical file, enabling your Doctor to make important comparisons if potential problems appear at future examinations.
Your Doctor strongly believes the OptoMap Retinal Exam is an essential part of your Comprehensive Eye Exam and highly recommends it for all patients every year. The entire retinal exam procedure will only take a few minutes and may eliminate the need for dilation.
